
Top 10 Mommy Makeover Frequently Asked Questions (FAQs)
The Mommy Makeover remains one of the most commonly performed Cosmetic Plastic Surgery Procedure combinations in the San Francisco Bay Area. Today, on the […]
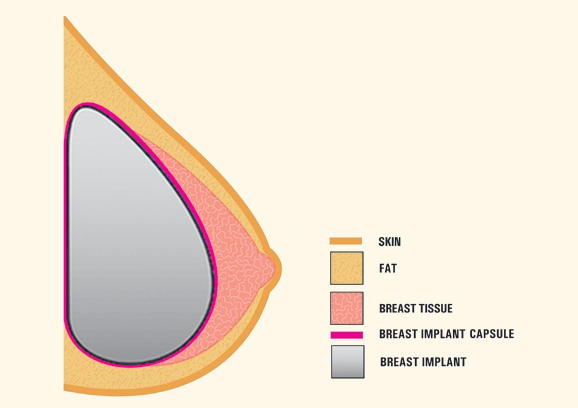
Statement on Breast Implant Capsulectomy Definitions 2024
Surgical treatment of breast implant capsules are varied and diverse. Today, I want to review the available options and outline when they are used. […]

Breast Implant Maintenance and Resizing
Breast Augmentation remains the most popular cosmetic plastic surgery. Whether placed for reconstructive or cosmetic reasons, Breast Implant Revision is needed from time to […]

Breast Implant Maintenance and Breast Revision Surgery
Breast Implants have come a long way over their 60 years of existence. They are available in a wider range of shapes, volumes and […]
Breast Implant Replacement Surgery
A week doesn’t go by without someone asking, “When do I need to replace my breast implants?” The simplest answer is, “When there’s a […]

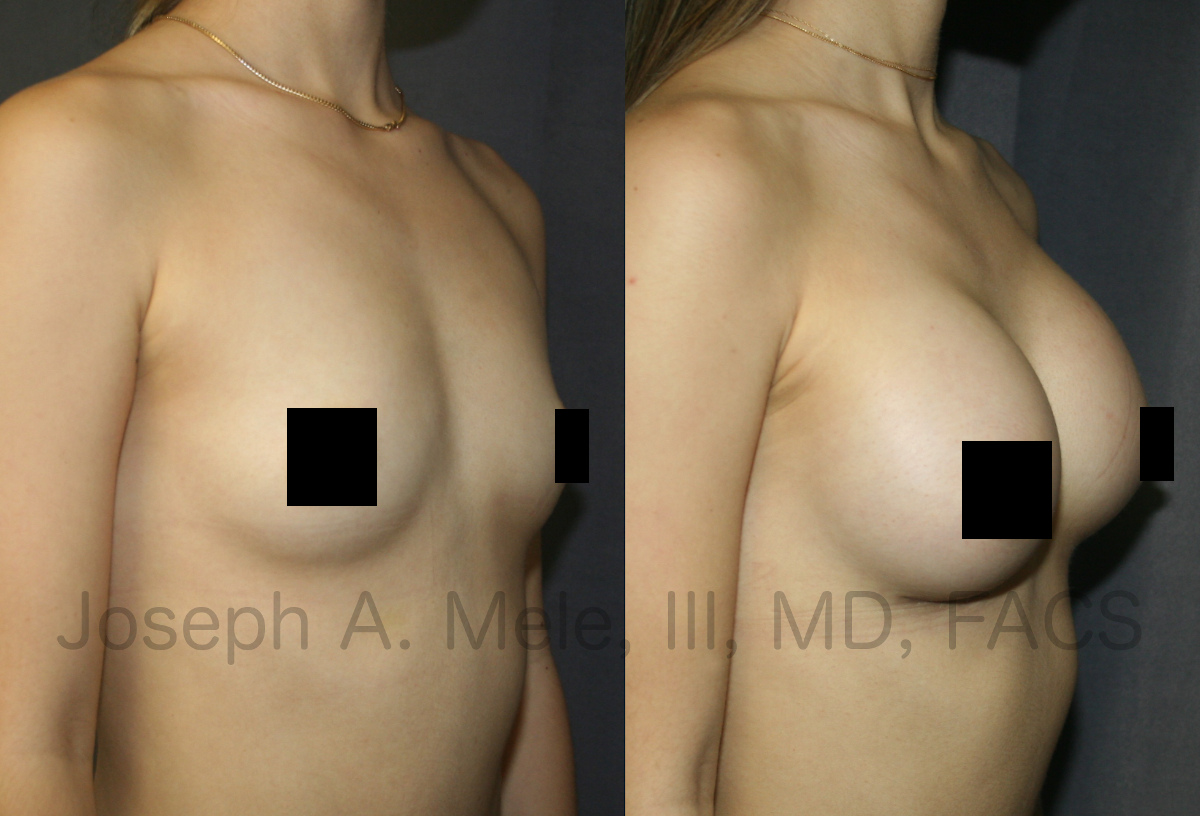
Breast Augmentation Revision Surgery Facts
Breast Augmentation remains one of the most requested Cosmetic Plastic Surgery procedures. It is important to remember that Breast Implants are not lifetime devices, […]

Breast Augmentation Revision Video Presentation – SF Bay Area
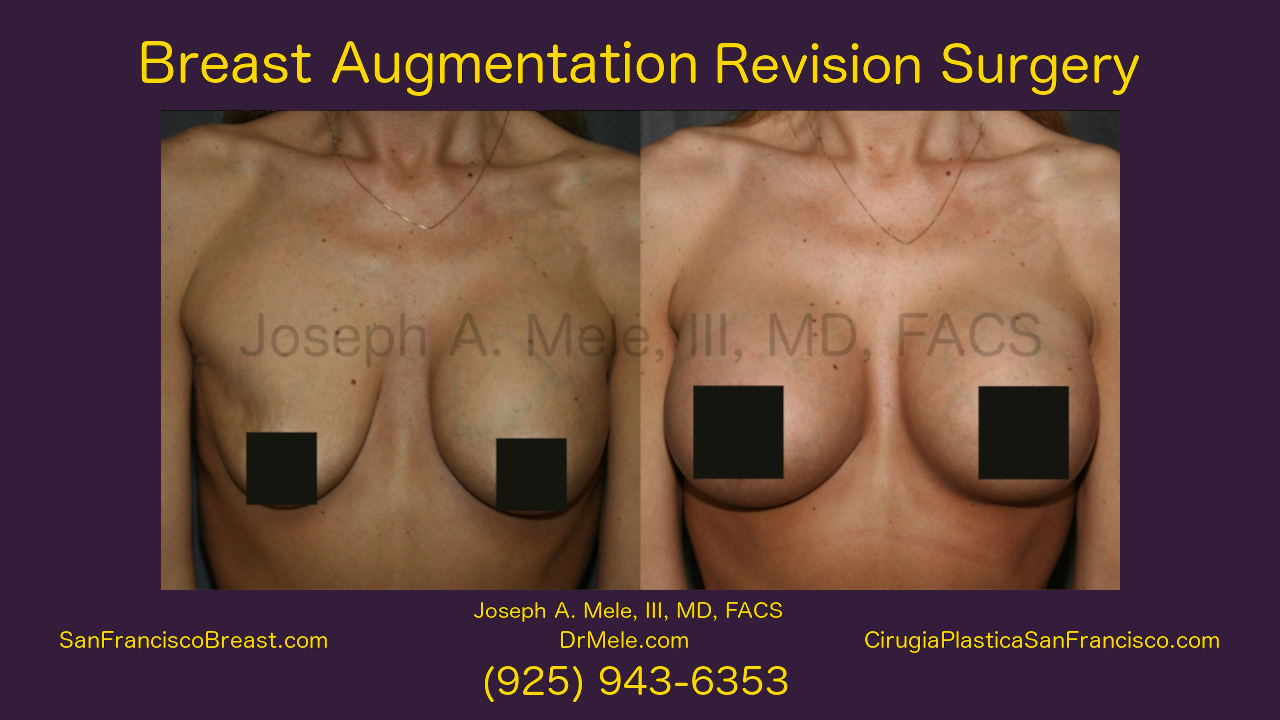
Breast Augmentation Revision Surgery restores and enhances the results of Breast Augmentation. Breast Implant Revision Surgery is used to change implant sizes, improve implant […]

Breast Augmentation Revision Surgery (Breast Implants)
Breast Augmentation sometimes requires maintenance. Breasts change over time, especially with pregnancy and fluctuations in weight, and your breast augmentation may need an occasional […]

Breast Augmentation on Body Beautiful (Breast Implants)
Breast Augmentation with Breast Implants The safest and most predictable way to enhance the size of your breasts remains Breast Augmentation with Breast Implants. […]
Breast Revision Surgery Video
Breast Augmentation remains one of the most frequently performed cosmetic plastic surgery operations. While the procedure remains the safest and most reliable means of […]