Breast Implant Replacement Surgery
A week doesn’t go by without someone asking, “When do I need to replace my breast implants?” The simplest answer is, “When there’s a […]

Happy Patient = Happy Plastic Surgeon
It is an honor and a blessing to be a plastic surgeon. I get to practice medicine, one of the most challenging and stimulating […]
Spring Breast Augmentation. Which Breast Implants?
Spring is definitely in the air. The first day of Spring is this Friday, March 19th, and as winter winds down, the demand for […]
Gummy Bear Breast Implants
Gummy Bear Breast Implants – Breast Implant Manufacturers don’t like the nickname, and I imagine neither do the folks at Haribo who make Gummi […]

Breast Implant Revision Surgery Breast Augmentation Revision Video
Breast Augmentation Revision Surgery restores and corrects the appearance of Breast Implants that are not satisfactory. When Breast Implants deflate, move or become hard, […]

Breast Augmentation Revision Surgery Facts
Breast Augmentation remains one of the most requested Cosmetic Plastic Surgery procedures. It is important to remember that Breast Implants are not lifetime devices, […]

FDA Updates Breast Implant Requirements
Breast Implants are the most investigated and regulated medical device in all of human history. As a Board Certified Plastic Surgeon who has participated […]

Breast Augmentation Revision Surgery (Breast Implants)
Breast Augmentation sometimes requires maintenance. Breasts change over time, especially with pregnancy and fluctuations in weight, and your breast augmentation may need an occasional […]
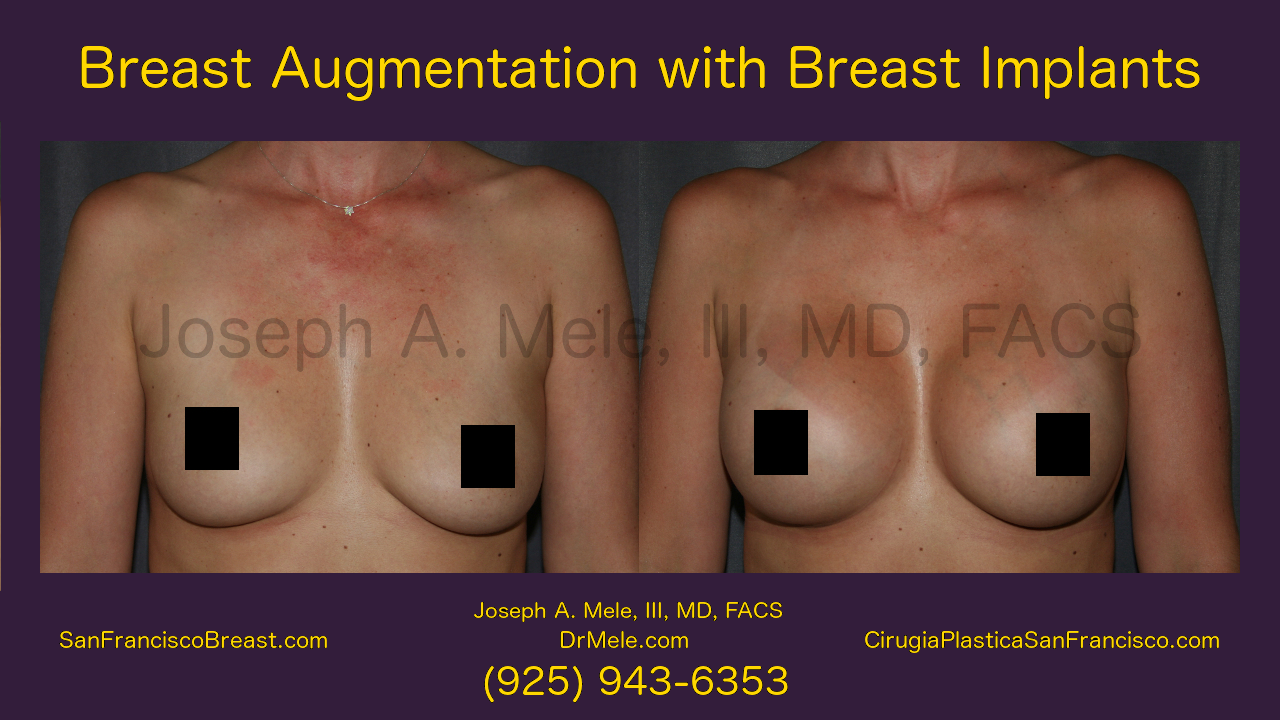
Breast Augmentation Video Presentation
Breast Augmentation remains the most popular cosmetic plastic surgery procedure, and with the new gummy bear breast implants, Breast Enhancement has never been safer […]

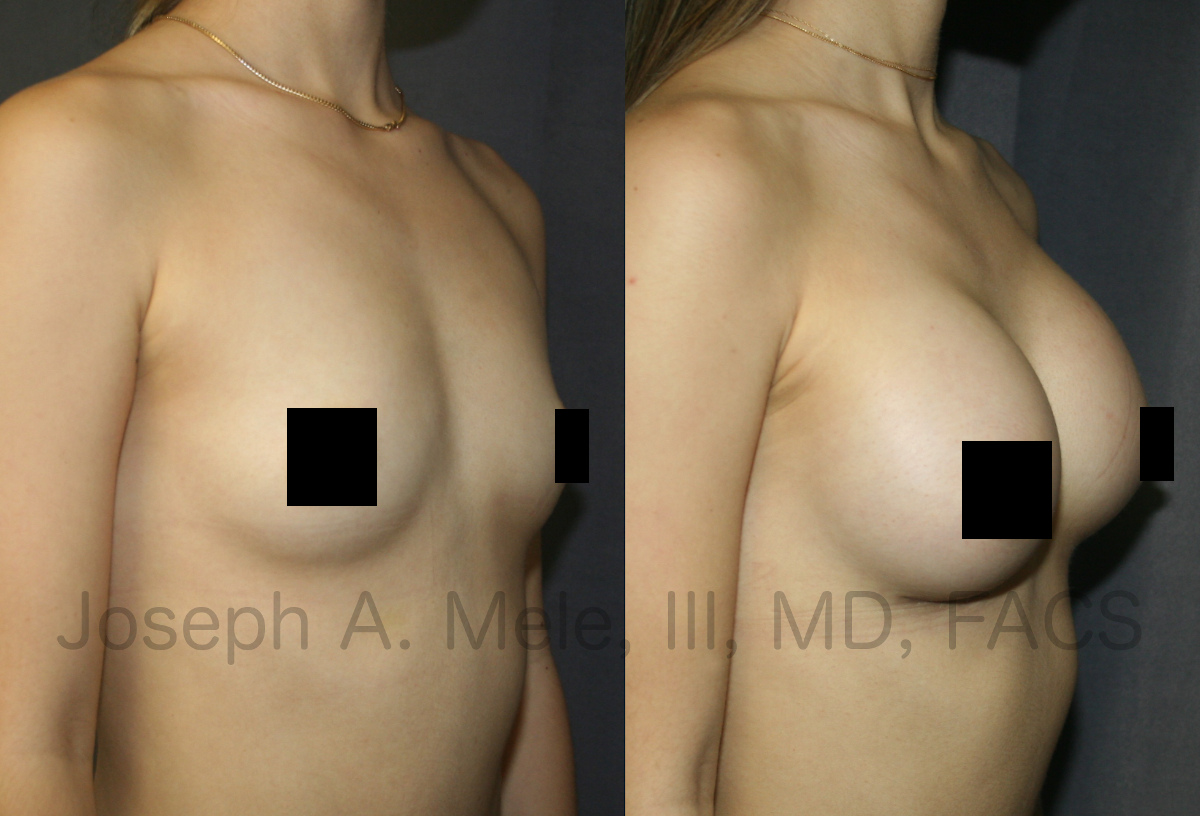
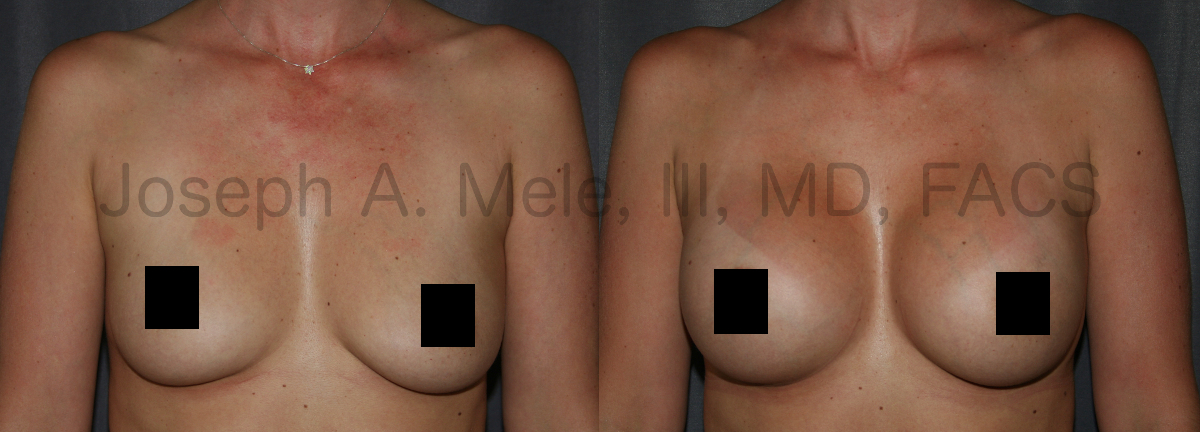
Breast Augmentation with Gummy Bear Breast Implants
Breast Augmentation remains one of the most popular cosmetic plastic surgery procedures. Today we are discussing Breast Augmentation with Gummy-Bear Breast Implants with before […]