
Inverted Nipple Repair and Nipple Reduction Surgery
Breast Asymmetry is more the rule than the exception. Size, shape and location of the breast mound all come into play; however, asymmetry may […]

Beyond The Before and After – Colby’s Story
Last year, the Aesthetic Society released the first season of Beyond the Before & After. Episode 4 featured a patient of mine who lost […]
Beyond the Before and After – The Aesthetic Society Reception
A few weeks back, I announced the release of the Aesthetic Society’s Beyond the Before and After. This week, a reception was held at […]

Daddy Makeover – Behind the Scenes at Beyond the Before and After
Last week’s post featured The Aesthetic Society’s Beyond the Before & After, featuring my patient who lost over 100 pounds and dramatically changed his […]
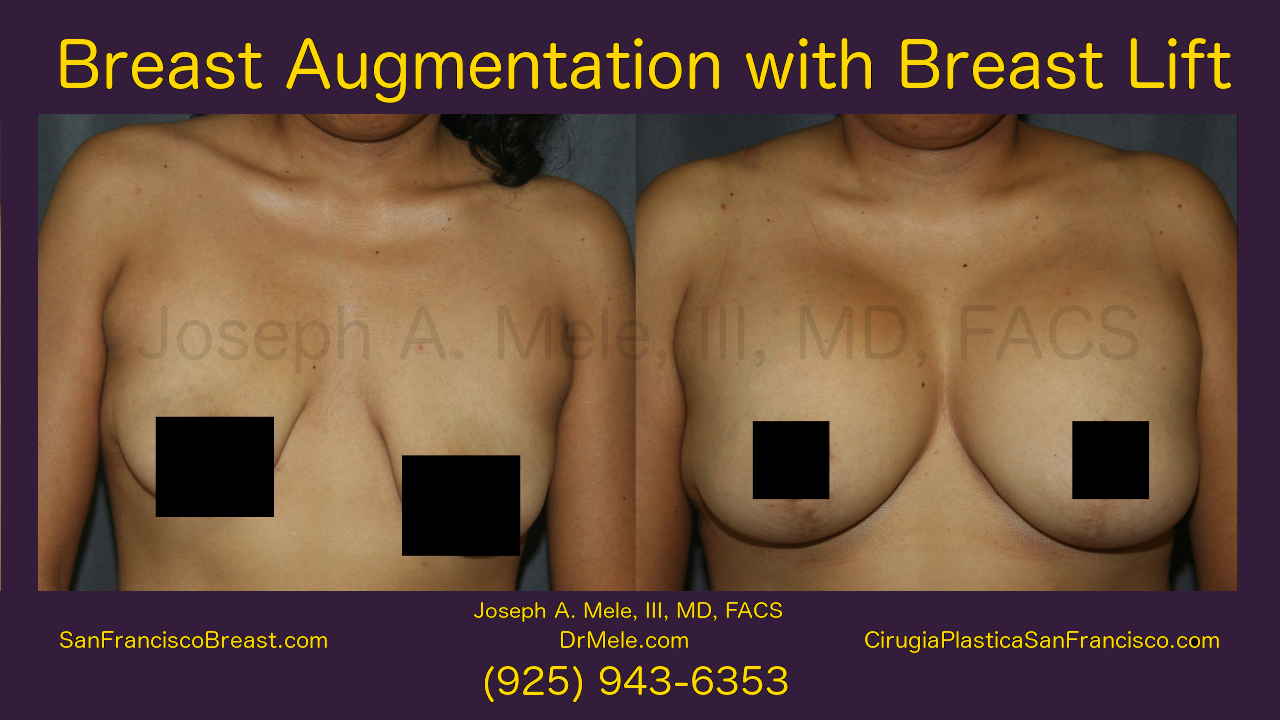
Breast Augmentation Lift Video Presentation
Breast Augmentation Lift Video Presentation Today’s Breast Implant with Breast Lift Video is from last week’s episode of Body Beautiful. This segment originally aired […]

Male Breast Reduction for Gynecomastia Video
Gynecomastia is the growth of excess breast tissue in the male chest. The resulting mass causes fullness, embarrassment and often tenderness, for men who […]
San Francisco Breast 2.0 Enhancement (Augmentation, Lift and Reduction)
New Breast Enhancement Content SanFranciscoBreast.com has been completely updated. This update includes new content, and it is artfully illustrated with new breast enhancement videos […]

Body Beautiful is Featuring Breast Implants Bay Area
To celebrate the debut of the new San Francisco Breast dot com (SanFranciscoBreast.com), a site dedicated to cosmetic breast surgery for the San Francisco […]

SanFranciscoBreast.com – A New Site Dedicated to Cosmetic Breast Surgery
San Francisco plastic surgery patients have an extensive new local resource encompassing all aspects of cosmetic breast enhancement surgery. I have consolidated my years […]
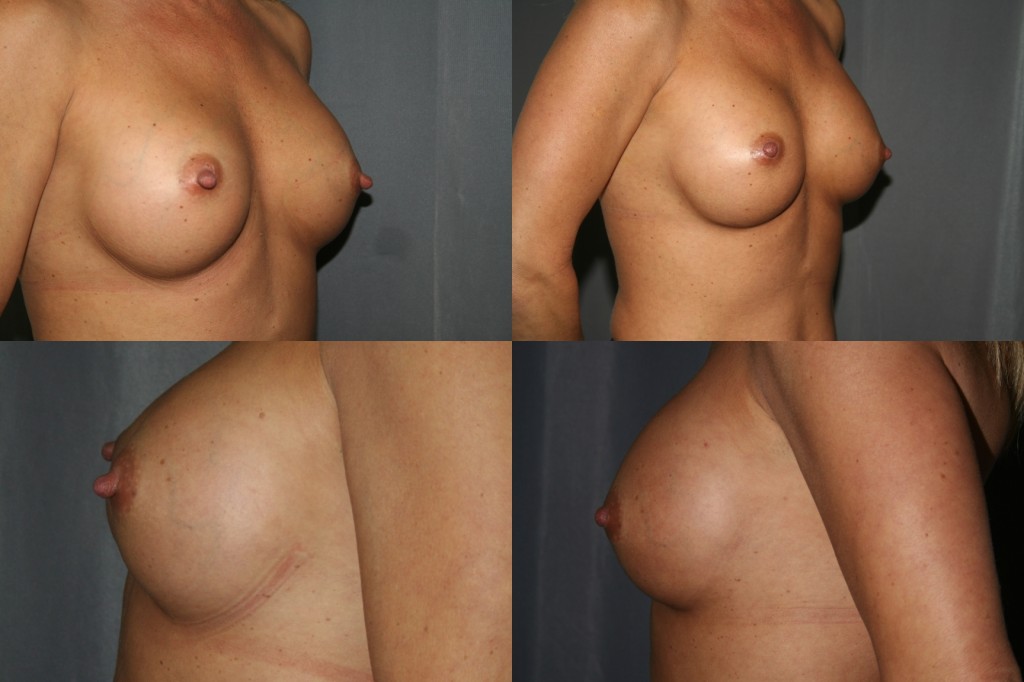
Breast Augmentation Revision Surgery
Breast augmentation has become the most frequently performed cosmetic plastic surgery procedure. As a result, breast augmentation revision has also increased. This topic has […]