
Gynecomastia Reduction for Enlarged Male Breasts
Winter is a great time for Breast Reduction. You can recover while covered up and enjoy the results this summer as the weather warms […]
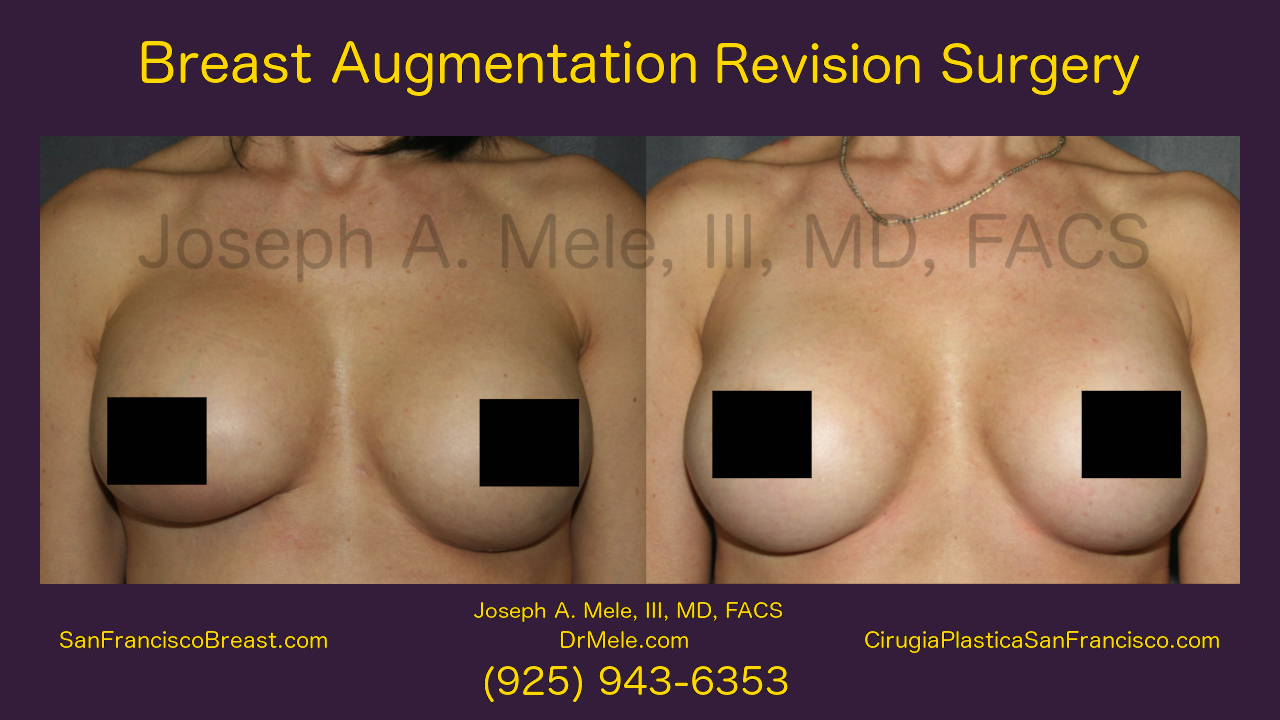
Breast Augmentation (Implant) Revision Surgery
Breast Implants have been used to enlarge breasts for over 50 years. Proper placement of the Breast Implants is the key to optimal Breast […]

Male Breast Reduction for Gynecomastia Video
Gynecomastia is the growth of excess breast tissue in the male chest. The resulting mass causes fullness, embarrassment and often tenderness, for men who […]

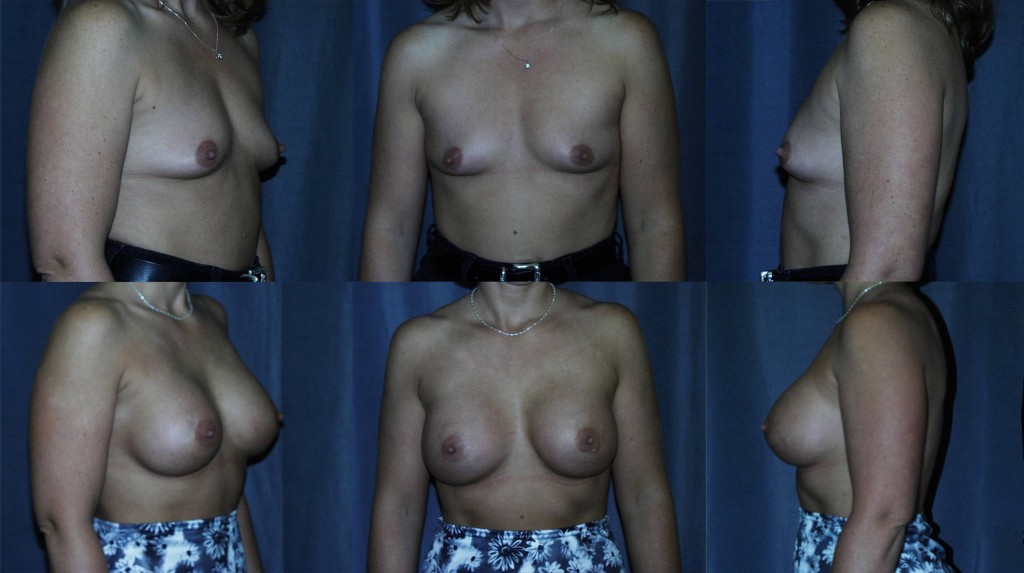
Breast Augmentation Before and Afters
Year after year, Breast Augmentation remains the most popular cosmetic plastic surgery procedure in the United States. This is true in the San Francisco […]
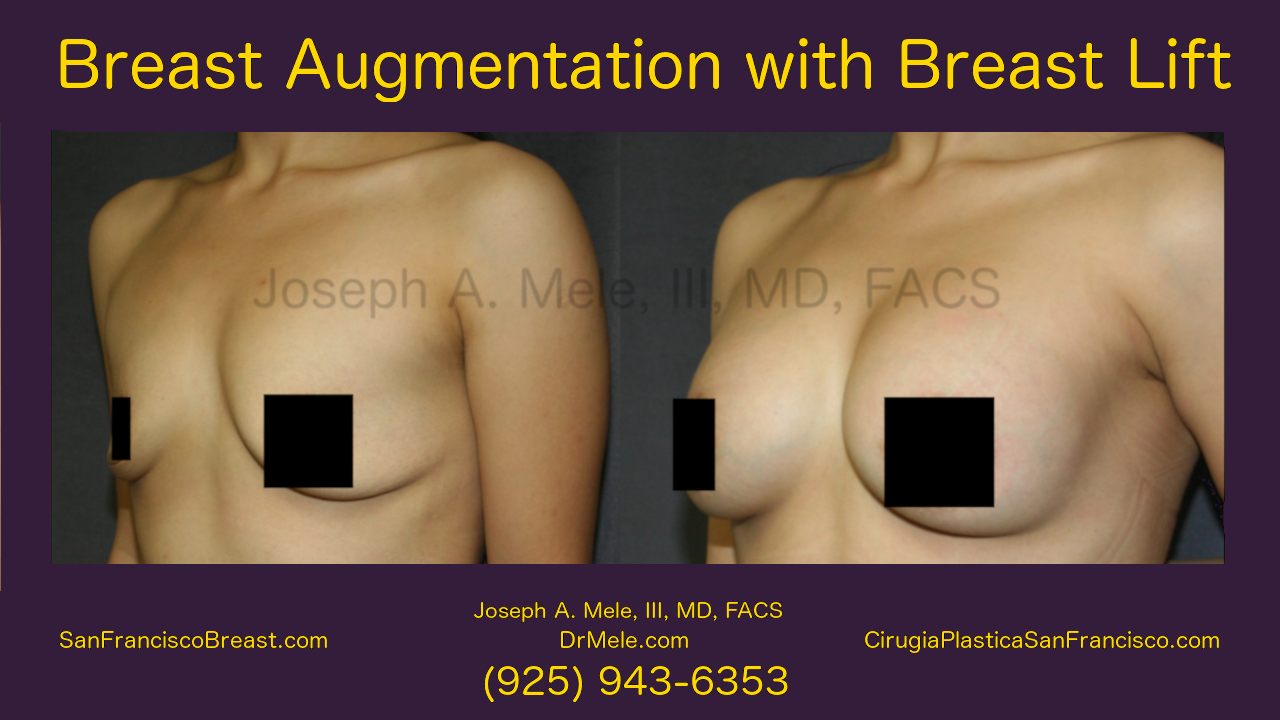
Breast Augmentation With A Breast Lift (Video Presentation)
The Components Of Breast Enhancement Breast Enhancement surgery has two aesthetic components: size and shape. Breast size is increased with Breast Augmentation and reduced […]
San Francisco Breast 2.0 Enhancement (Augmentation, Lift and Reduction)
New Breast Enhancement Content SanFranciscoBreast.com has been completely updated. This update includes new content, and it is artfully illustrated with new breast enhancement videos […]

When Breast Augmentation Needs A Lift
Mastopexy Augmentation is the combination of Breast Augmentation and Breast Lift. When is Breast Augmentation alone enough? When is a Breast Lift the best […]
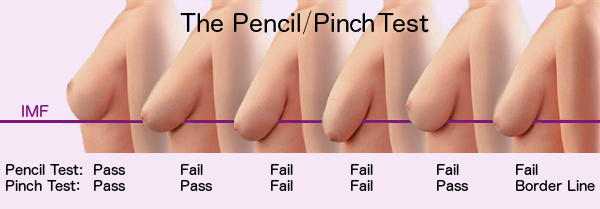
Do I Need A Breast Lift? The Pencil Test vs. The Pinch Test
One of the most frequent questions I get during a Breast Augmentation consultation is, “Do I need a breast lift?” The decision is based […]
Tubular Breasts and Plastic Surgery – Walnut Creek, San Francisco East Bay Area
Tubular breast deformity is a common, congenital breast abnormality found in both women and men. In men, the treatment is straight forward (see the […]

SanFranciscoBreast.com – A New Site Dedicated to Cosmetic Breast Surgery
San Francisco plastic surgery patients have an extensive new local resource encompassing all aspects of cosmetic breast enhancement surgery. I have consolidated my years […]