
Breast Implant Maintenance and Breast Revision Surgery
Breast Implants have come a long way over their 60 years of existence. They are available in a wider range of shapes, volumes and […]
Breast Implant Replacement Surgery
A week doesn’t go by without someone asking, “When do I need to replace my breast implants?” The simplest answer is, “When there’s a […]

Breast Implant Revision Surgery Breast Augmentation Revision Video
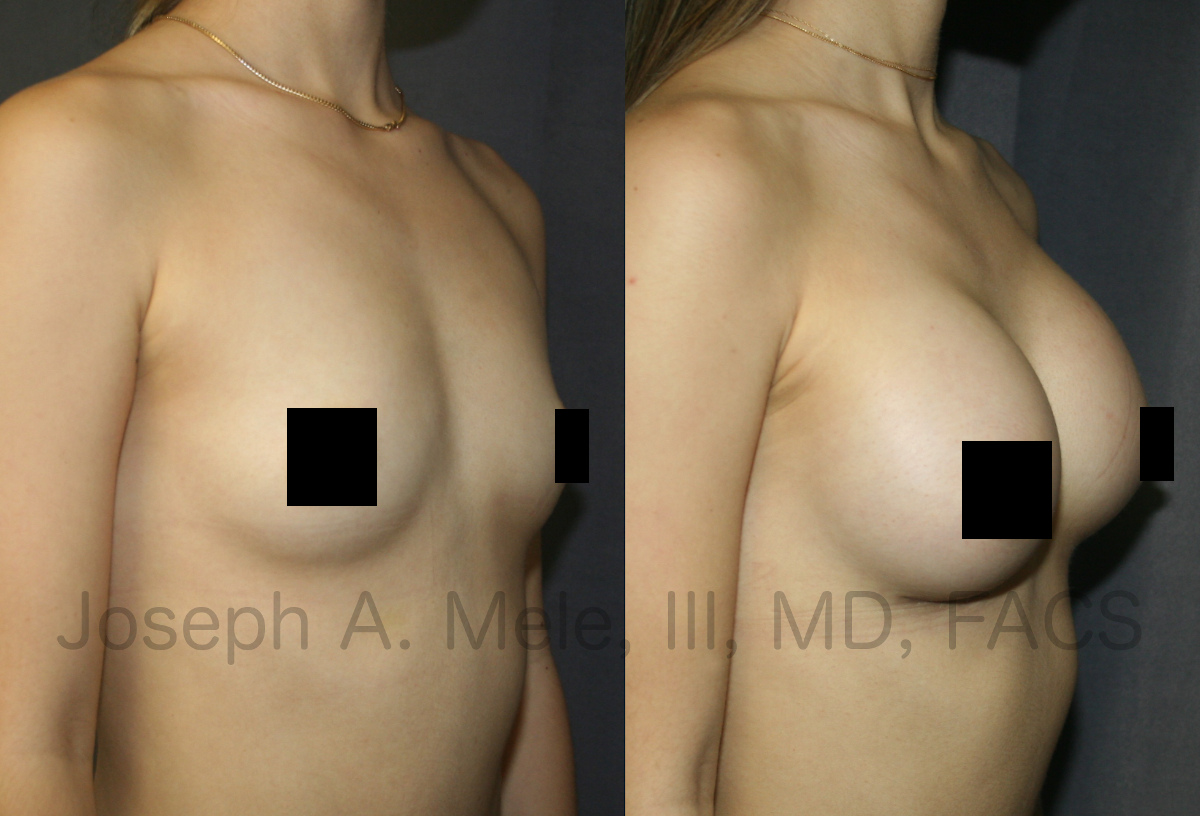
Breast Augmentation Revision Surgery restores and corrects the appearance of Breast Implants that are not satisfactory. When Breast Implants deflate, move or become hard, […]

Breast Augmentation Revision Surgery Facts
Breast Augmentation remains one of the most requested Cosmetic Plastic Surgery procedures. It is important to remember that Breast Implants are not lifetime devices, […]

Breast Augmentation Revision Surgery (Breast Implants)
Breast Augmentation sometimes requires maintenance. Breasts change over time, especially with pregnancy and fluctuations in weight, and your breast augmentation may need an occasional […]

Breast Augmentation with Gummy Bear Breast Implants
Breast Augmentation remains one of the most popular cosmetic plastic surgery procedures. Today we are discussing Breast Augmentation with Gummy-Bear Breast Implants with before […]

Capsular Contracture Treatment – Breast Augmentation Revision Surgery
Capsular Contracture accounts for about one third of all Breast Augmentation Revision surgeries. But what is Capsular Contracture? How can it be prevented, and […]

Breast Augmentation Revision Surgery
Breast Implant Revision Surgery is performed when there is a problem with the breast implants. Some problems are subjective, for example when the implants […]

New Body Beautiful From Head to Tummy
Hey San Francisco Bay Area. Body Beautiful will be broadcast this Tuesday, September 12, at noon. You may not have noticed, but KRON 4 […]
San Francisco Breast 2.0 Enhancement (Augmentation, Lift and Reduction)
New Breast Enhancement Content SanFranciscoBreast.com has been completely updated. This update includes new content, and it is artfully illustrated with new breast enhancement videos […]