
Mommy Makeovers – Breast and Belly Rejuvenation
There is no denying that breasts and bellies take a hit with pregnancy. Fortunately, there is a solution. Mommy Makeovers rejuvenate both the breasts […]

Massive Gynecomastia Reductions (Video Presentation)
Gynecomastia Reduction is one of the most frequently performed cosmetic plastic surgery procedures for men. Over the last 20 years, the number of Gynecomastia […]
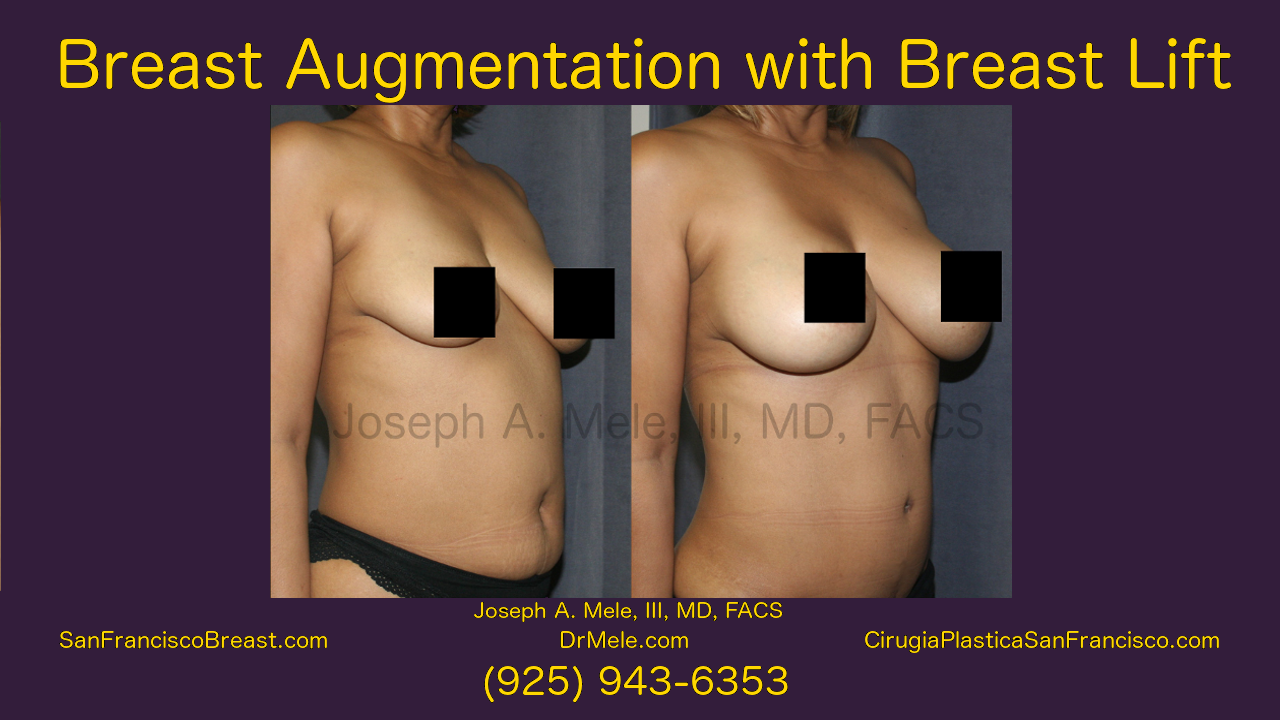
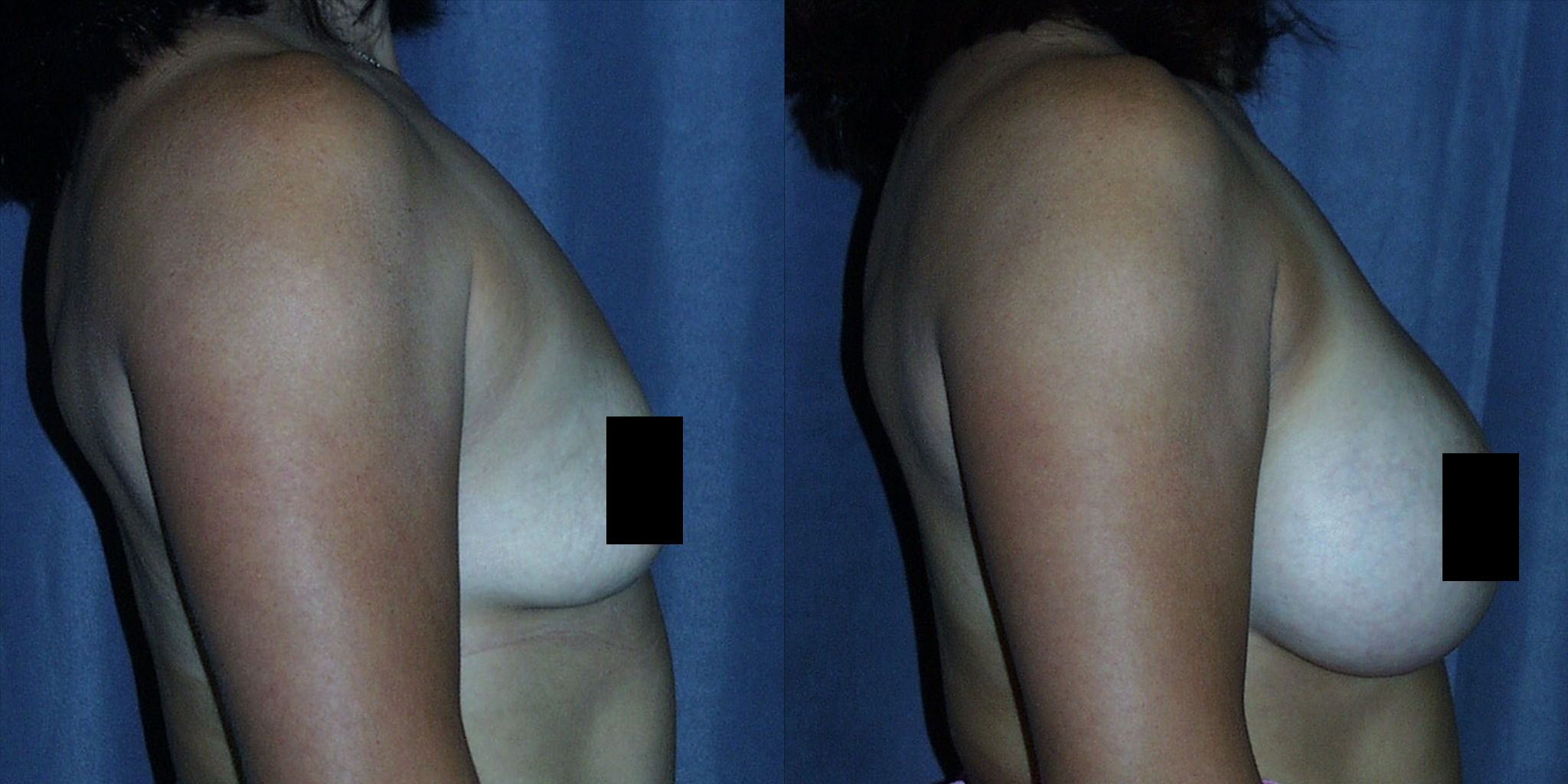
Breast Augmentation and Breast Lifts (Video Presentation)
Aesthetic Breast Surgery The desire for the Best Breast can be divided into two areas: The best size and the best shape. This Breast […]
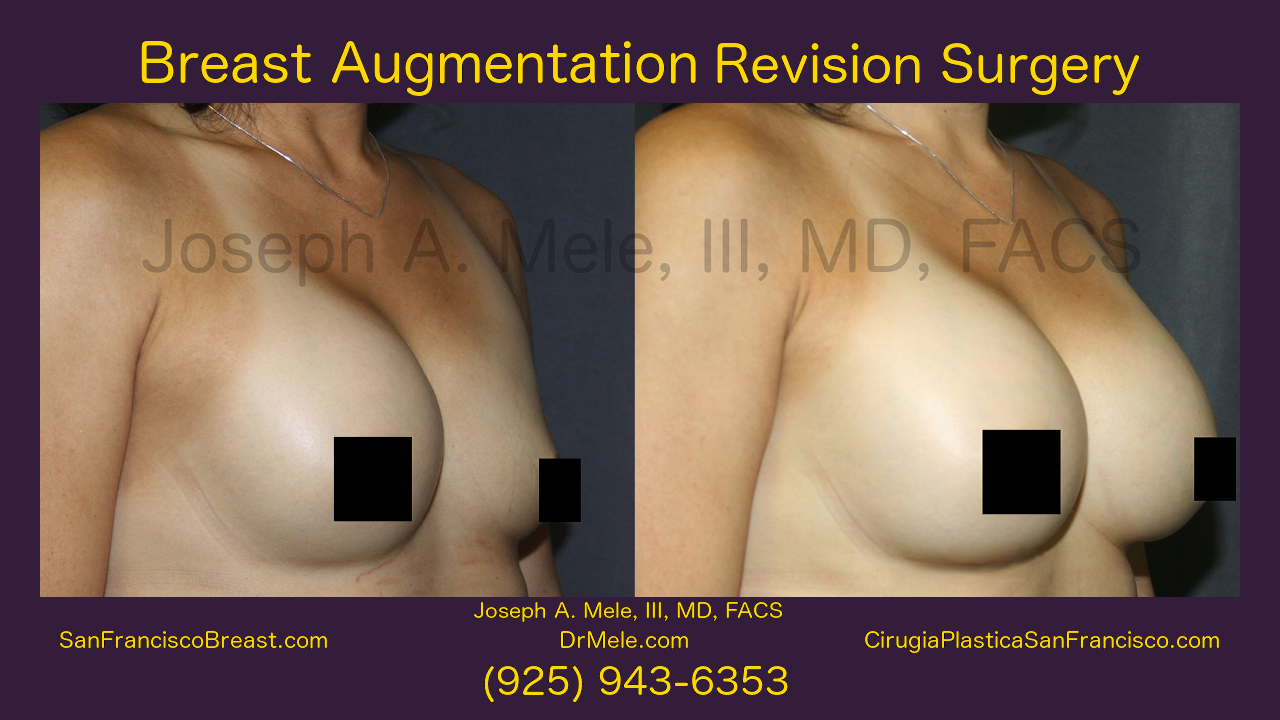
Breast Implant Revision Video Presentation
Breast Augmentation with Breast Implants remains the most popular cosmetic plastic surgery. Three to four-hundred-thousand women have Breast Augmentation each year in the US […]
San Francisco Breast 2.0 Enhancement (Augmentation, Lift and Reduction)
New Breast Enhancement Content SanFranciscoBreast.com has been completely updated. This update includes new content, and it is artfully illustrated with new breast enhancement videos […]

Breasts, Belly and Bootie Lifts – SF Bay Area Plastic Surgery
This Wednesday, June 7, 2017, I will be on the San Francisco Bay Area’s News Station, KRON 4’s Body Beautiful. The show airs live […]
Fat Grafting and Breast Augmentation – Part 3 of 3
Is Fat Grafting Experimental Surgery? Fat Grafting has been around for at least 125 years, so it is not an experimental surgery. However, the […]

Fat Grafting and Breast Augmentation – Part 2 of 3
Fat Grafting Today Like most Board Certified Plastic Surgeons, I perform fat grafting for selected patients. Facial Augmentation, Brazilian Butt Lifts and to help […]
Fat Grafting and Breast Augmentation – Part 1 of 3
Many of my San Francisco Plastic Surgery Blog posts are inspired by the questions I get from patients. Inquires come from patients in my […]

What is Breast Implant Capsular Contracture?
Breast Augmentation remains the most popular cosmetic plastic surgery procedure year after year. Breast Implants enlarge small breasts, whether you were born with small […]