
Breast Augmentation Revision Surgery (Breast Implants)
Breast Augmentation sometimes requires maintenance. Breasts change over time, especially with pregnancy and fluctuations in weight, and your breast augmentation may need an occasional […]

Breast Augmentation with Gummy Bear Breast Implants
Breast Augmentation remains one of the most popular cosmetic plastic surgery procedures. Today we are discussing Breast Augmentation with Gummy-Bear Breast Implants with before […]

Breast Augmentation with a Breast Lift (Mastopexy Augmentation)
For the best cosmetic result, sometimes Breast Enhancement requires both enlargement and lifting. When performed together, the procedure is known as a Mastopexy Augmentation. […]
Breast Augmentation Revision for Symmastia (Uniboob)
Symmastia is a type of Breast Implant Malposition which occurs when the implants are too close together. When the implants slide across the midline […]
Breast Revision Surgery Video
Breast Augmentation remains one of the most frequently performed cosmetic plastic surgery operations. While the procedure remains the safest and most reliable means of […]

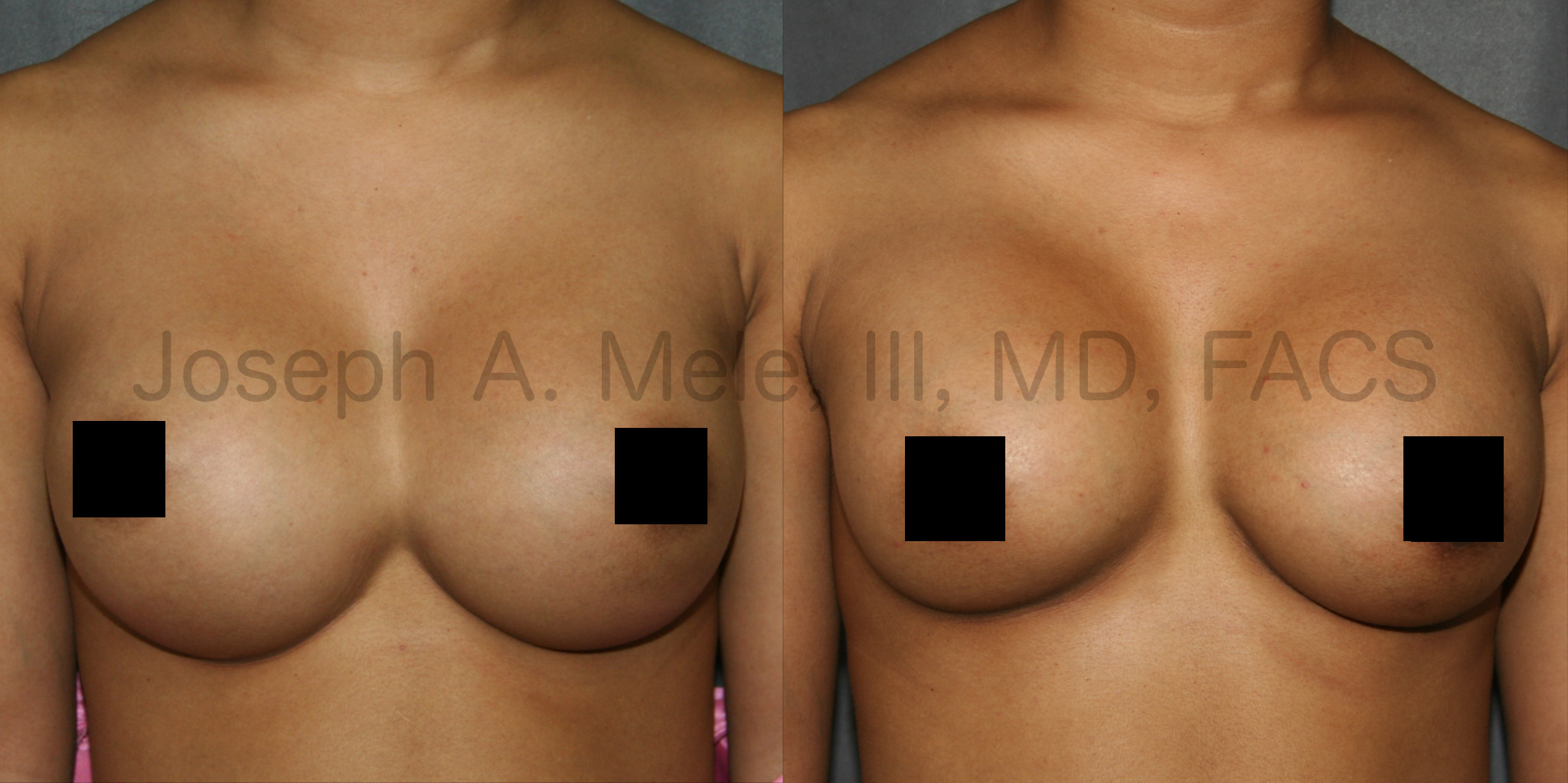
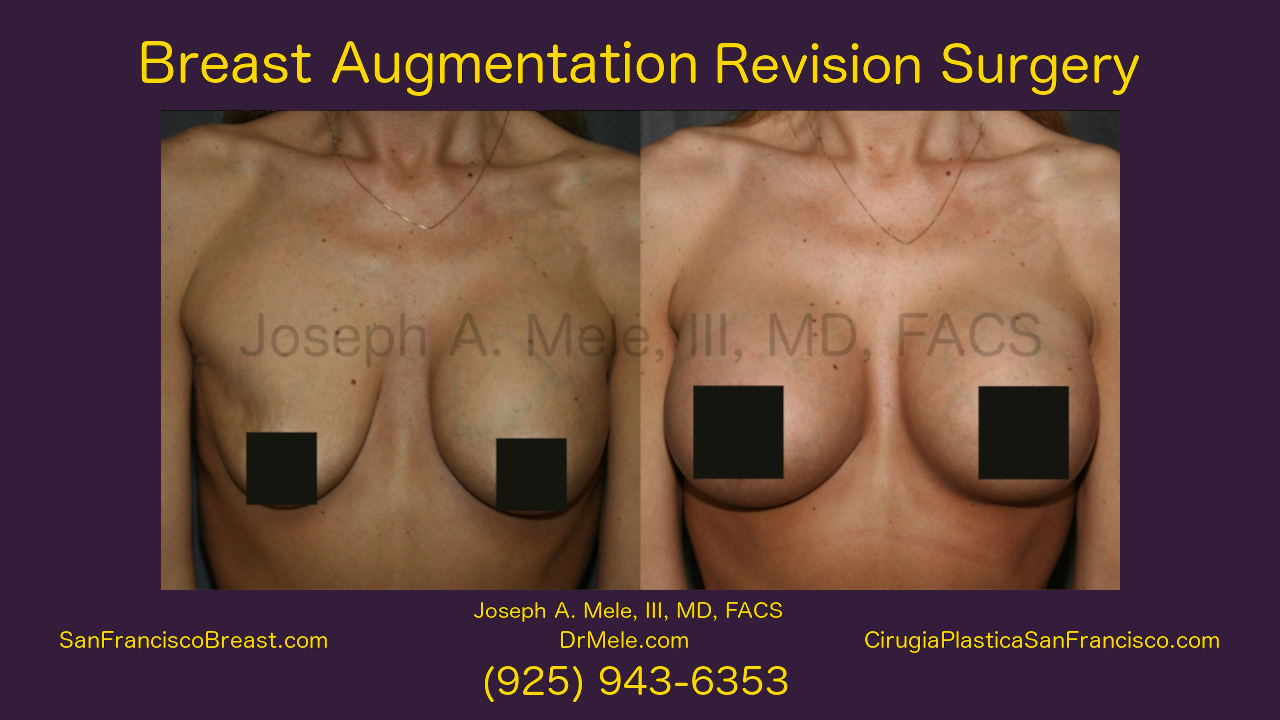
Breast Augmentation Revision Surgery
Breast Implant Revision Surgery is performed when there is a problem with the breast implants. Some problems are subjective, for example when the implants […]

Breast Implant Revision Before and After Pictures – Capsular Contracture
There are many different reasons for Breast Implant Revision Surgery. Possible causes include: Capsular Contracture Breast Implant Malposition: Too high Too Low (Bottoming out) […]

Male Breast Reduction for Gynecomastia Video
Gynecomastia is the growth of excess breast tissue in the male chest. The resulting mass causes fullness, embarrassment and often tenderness, for men who […]

Breast Augmentation Before and Afters
Year after year, Breast Augmentation remains the most popular cosmetic plastic surgery procedure in the United States. This is true in the San Francisco […]

Breast Augmentation With A Lift
For patients unhappy with their deflated, saggy breasts, Breast Augmentation is a common remedy. There are times, however, when Breast Enlargement alone may not […]