
Fleur De Lis Tummy Tuck – Post-Bariatric Plastic Surgery
Variety is the spice of life, and it is the single most important aspect of plastic surgery that makes my job both rewarding and […]
Areolar Reduction, Breast Asymmetry, Breast Augmentation, Breast Augmentation Lift, Breast Lift (Mastopexy), Home, Tubular Breasts
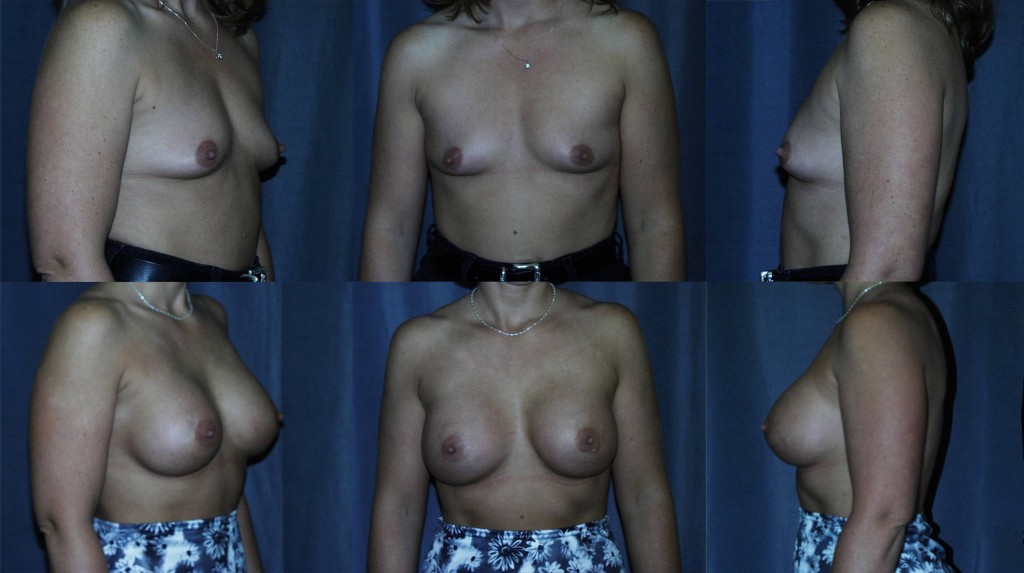
Tubular Breasts and Plastic Surgery – Walnut Creek, San Francisco East Bay Area
Tubular breast deformity is a common, congenital breast abnormality found in both women and men. In men, the treatment is straight forward (see the […]

Mammogram Recommendations – When to Start Routine Screening
Remember when the revised US Preventative Service Task Force (USPSTF) recommendations for breast cancer screening were released in November 2009? Like the recent FDA […]