
The Cosmetic Plastic Surgery Tax
Dear Patient, The Healthcare plan in the Senate today will unfairly discriminate against you. I’m writing you today about an issue that affects not […]

Hypertrophic Scar Revision San Francisco
The previous example of scar revision was a keloid scar revision. Keloid scars tend to be raised and larger than the original injury. The […]
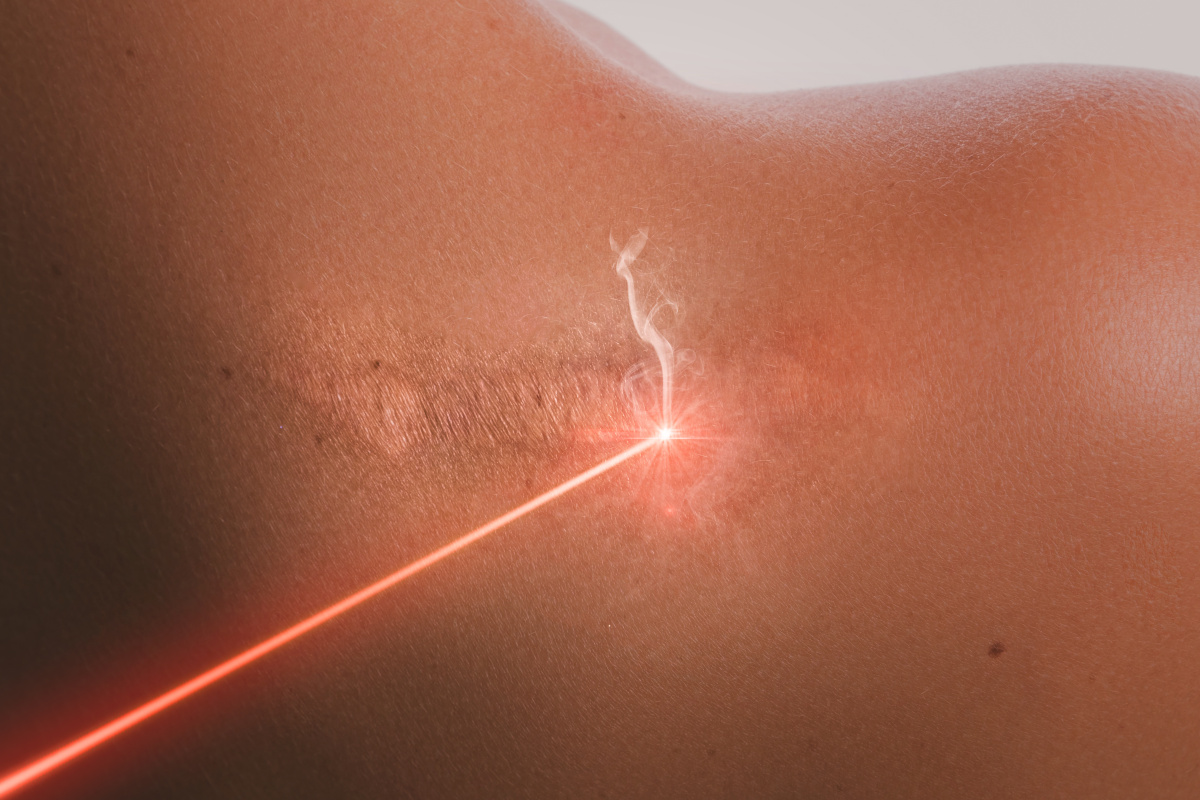
Scar Revision Treatment Options
How can hypertrophic and keloid scars be improved? What options are available to treat unsatisfactory scars? Here are some of the different scar treatments […]

Scar Revision – Scar Evaluation
The evaluation of a scar encompasses the following ten points, the first and last may be the most important. 1 – Time Since Injury […]

Keloid Scar San Francisco
Before I get into the details of how to evaluate a scar, I would like to provide a quick example of scar revision. Scars […]