
New Plastic Surgery Products – Dysport® vs. Botox®
There’s a new kid in town, at least for Walnut Creek plastic surgery. While Dysport® has been a mover and shaker Europe for years, […]
New Plastic Surgery Products – Summer 2009
The topic for this week is what’s new in plastic surgery. Cosmetic plastic surgery is always changing. We are constantly looking for new and […]

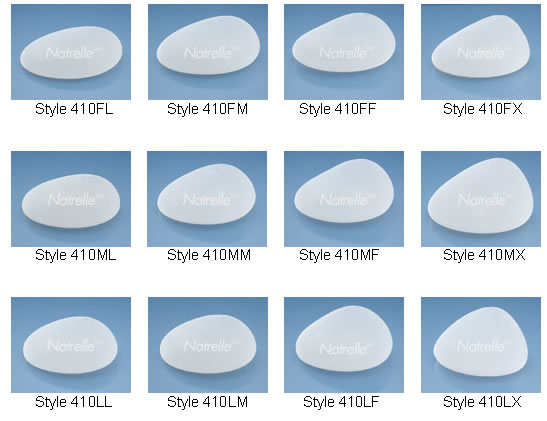
How to Choose the Correct Breast Implants: Silicone vs. Saline
So which filler is better Silicone or Saline? That has been the question since the introduction of the modern breast implants in the 1960’s. […]
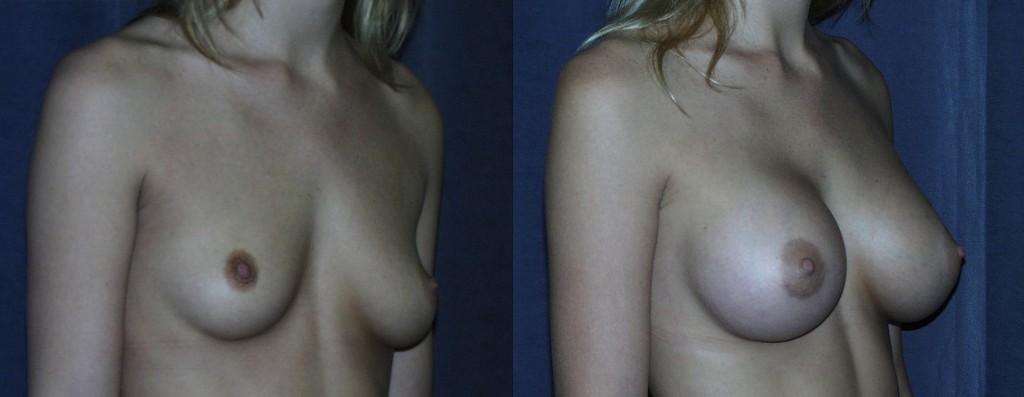
How to Choose the Correct Breast Implants: Size
If you are considering breast augmentation, size matters. Every day in my Walnut Creek cosmetic plastic surgery practice I get asked. “What breast implant […]
The Prevention and Treatment of Capsular Contracture after Breast Augmentation
Prevention How can we prevent capsular contracture? There is some evidence that bacteria may play a role in capsular contracture. Proper surgical technique, placement […]
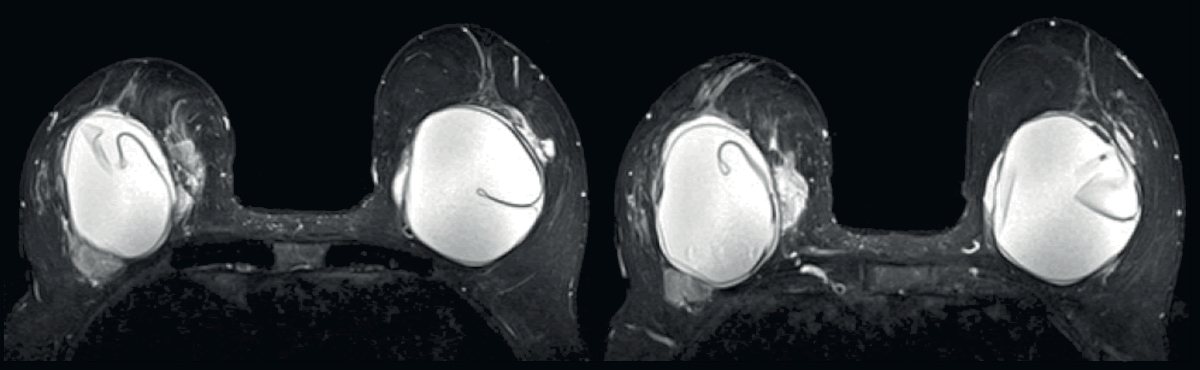
What is Capsular Contracture?
In response to questions asked about the case study of capsular contracture previously posted, I am expanding the information into a short three part […]
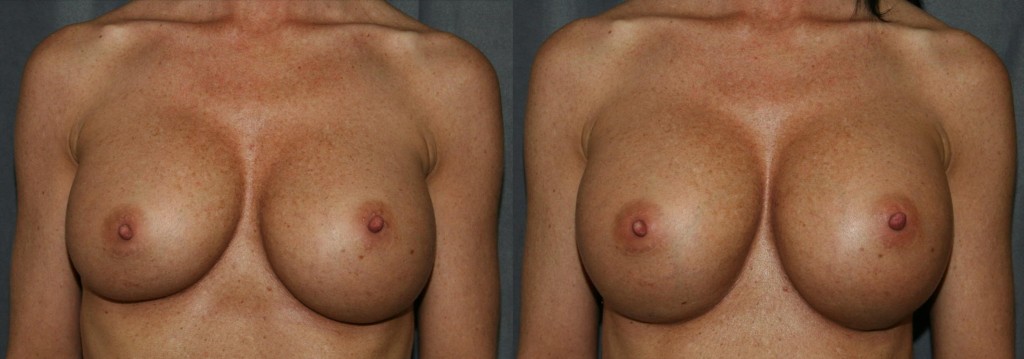
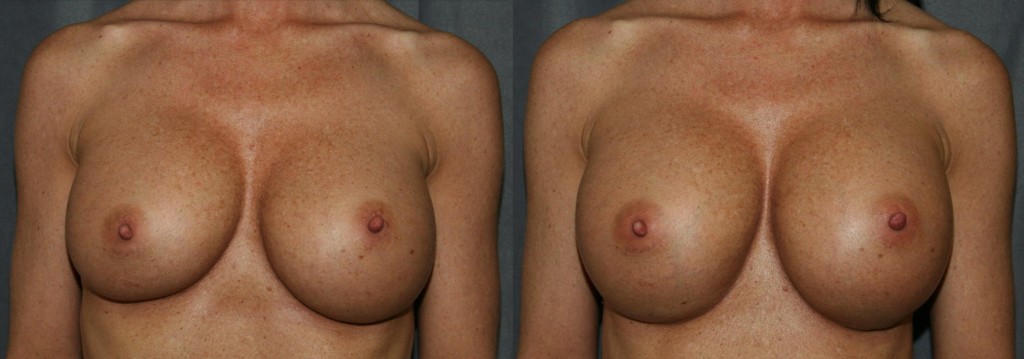
Breast Implant Revision Surgery: Capsular Contracture
Breast Implant Revision Surgery has become an important part of my Walnut Creek, CA, Plastic Surgery practice. Today’s post is a case presentation of […]